I recently read an article on the New York Times Well Blog about a study in the Scandinavian Journal of Medicine & Science in Sports. The study, by Michael Rathleff and colleagues, compared strengthening vs. stretching exercises to treat plantar fasciitis (PF). In a nutshell, the Times article reported that the study found strengthening exercises to provide superior improvement after 3 months compared to stretching, but that with additional time the stretching group responded equally well compared to the strengthening group. So the basic conclusion might be interpreted as being that both interventions improved symptoms over the long term, but that foot strengthening exercises improve PF symptoms more rapidly.
Having experienced a long-term (though fairly low-grade) case of plantar fasciitis myself a few years ago, I’m always curious when I see reports of potentially effective treatment protocols for the condition. As such, I though I’d dig a bit more into this study.
The full text is not available for free (I received a copy from the author), but the lead author wrote up a nice summary of what they did on RunningPhysio.com. Basically, they took 48 patients with diagnosed plantar fasciitis and randomized them into either a plantar-specific stretching regimen or a high load strength training regimen for the foot (all subjects also received gel heel inserts).
Here’s the description of the stretching regimen (via Michael Rathleff on RunningPhysio):
“Patients were instructed to perform this exercise whilst sitting by crossing the affected leg over the contralateral leg (Figure 1). Then, while using the hand on the affected side, they were instructed to place the fingers across the base of the toes on the bottom of the foot (distal to the metatarsophalangeal joints) and pull the toes back toward the shin until they felt a stretch in the arch of the foot. They were instructed to palpate the plantar fascia during stretching to ensure tension in the plantar fascia. As in Digiovanni, patients were instructed to perform the stretch 10 times, for 10 seconds, three times per day [10].”

The above-described plantar fascia stretching regimen was used in a previous study (DiGiovanni et al., 2003) and was found to provide superior results to an Achilles tendon stretching regimen.
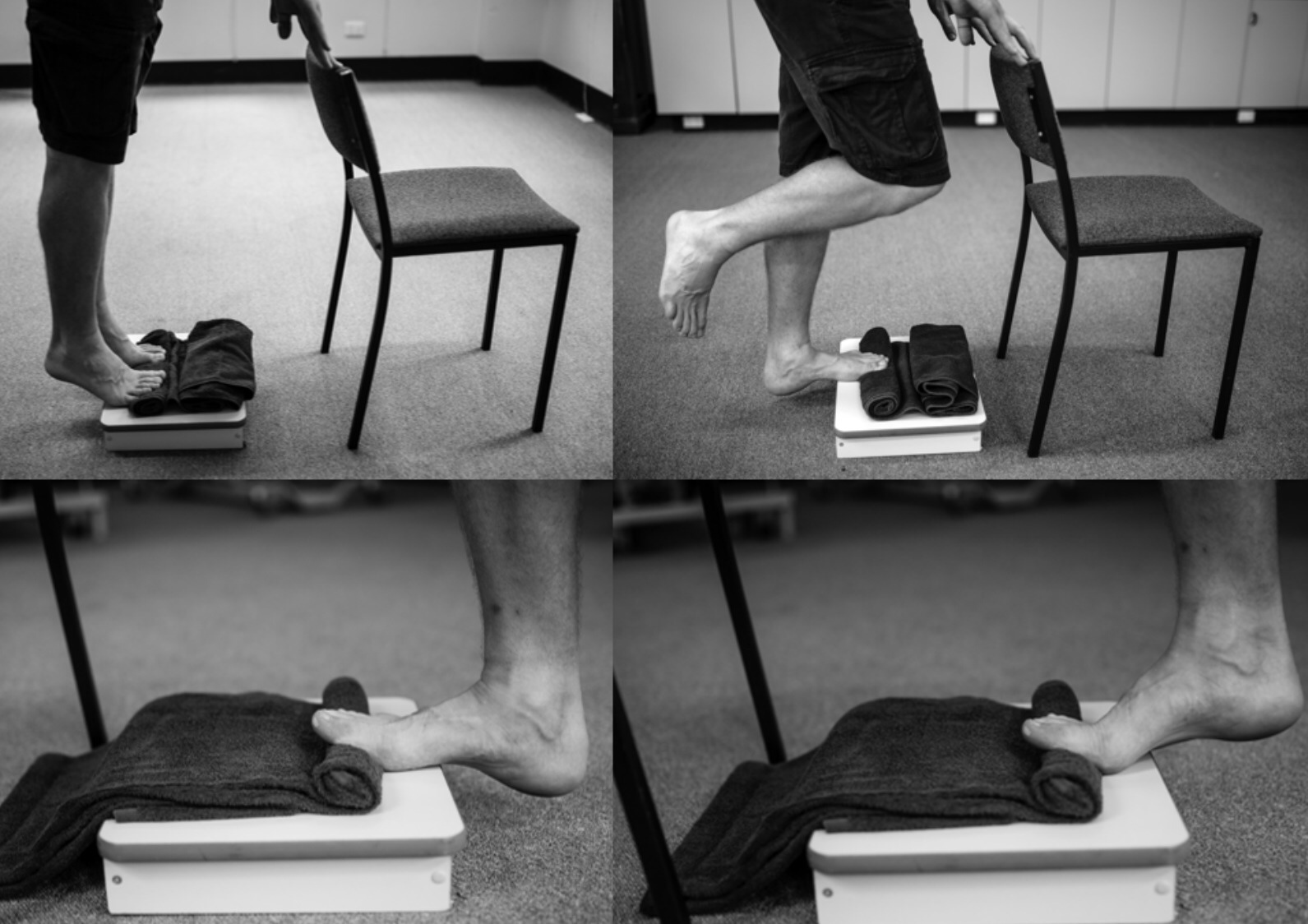
Here’s the description of the strengthening regimen (via Michael Rathleff on RunningPhysio):
“High-load strength training consisted of unilateral heel-raises with a towel inserted under the toes to further activate the windlass-mechanism (Figure 2). The towel was individualised, ensuring that the patients had their toes maximally dorsal flexed at the top of the heel-rise. The patients were instructed to perform the exercises every second day for three months. Every heel-rise consisted of a three second concentric phase (going up) and a three second eccentric phase (coming down) with a 2 second isometric phase (pause at the top of the exercise). The high-load strength training was slowly progressed throughout the trial as previously reported by Kongsgaard et al. [11]. They started at 12 repetition maximum (RM) for three sets. After two weeks, they increased the load by using a backpack with books and reduced the number of repetitions to 10RM, simultaneously increasing the number of sets to four. After four weeks, they were instructed to perform 8RM and perform five sets. They were instructed to keep adding books to the backpack as they became stronger.”
And here is the summary of study outcomes that the lead study author wrote on RunningPhysio:
We used the Foot Function Index as our primary outcome after three months but also did follow-ups after 1,6 and 12 months. At our 3 months follow-up we saw that patients randomised to high load strength training had a 29 points lower Foot Function Index. This is far greater than the minimal relevant difference and suggests a superior effect of high-load strength training compared to plantar specific stretching. An important aspect is that we saw no difference between groups at 6 and 12 months indicating no superior long-term effect. However, if you ask patients to choose between two treatments that have similar long-term effect but one will give you a quicker reduction in pain, I am certain that all patients would choose the treatment, which provides them with the quickest reduction in pain.
This all sounds great – if you have plantar fasciitis and want to improve your symptoms, a foot strengthening routine like the one used in this study could provide relief more quickly than a stretching routine. There is some logic behind this finding as eccentric loading is commonly used to treat tendon injuries such as in Achilles tendinopathy. The idea is that if you strengthen the tissue, it becomes better capable of handling the loads placed on it.
As with any academic study, it’s always important to be open minded and critical. Such is the nature of science. Podiatrist Craig Payne recently wrote a critique of this study on his site Run Research Junkie, and it makes for interesting reading. He points out that the results are consistent with the approach he advocates for treating plantar fasciitis, and outlines a number of positives about the study. But he also points out a number of concerns. Of these, I’m only going to comment on one here, and that is the lack of a control group that did not receive either intervention (or the gel heel inserts).
As Craig points out in his critique it is not atypical for plantar fasciitis to simply improve on its own with time (sometimes an extended period of time). For example, I experienced symptoms with my case of PF for over a year, and though I did seek treatment I have no idea if my case resolved due to a specific intervention (e.g., I did a lot of calf foam rolling, Graston/ART, and some stretching) or if it simply resolved on its own (it actually improved during a summer when I was running a lot more miles than I had in quite awhile). Thus, without a control group in this study we can’t say for certain that stretching or strengthening exercises performed better than just letting the case of PF improve with time (it’s worth noting that studies looking at the effectiveness of stretching vs. controls for treating PF have given mixed results). Craig also points out that the intervention of the gel heel insert in both groups could have contributed to improvement, but again we cannot assess any influence of that compared to a group that did not receive a heel insert.
All we can really say with certainty from this study is that foot strengthening exercises provided quicker improvement in plantar fasciitis symptoms when compared to plantar stretching. It’s important to note that this does not preclude either of these interventions as potentially valuable tools in the treatment of plantar fasciitis. It’s also worth noting that plantar stretching is a commonly used/advocated approach to managing plantar fasciitis, so in that sense this study was comparing a new protocol to one that is commonly used. As such, the fact that strengthening led to quicker improvement in symptoms is a valuable finding. But I do agree with Craig in that the lack of a control group makes it difficult to discern the benefit of either protocol relative to doing nothing at all. A logical follow-up study would therefore be to compare foot strengthening exercises to a sham treatment or no treatment at all.
All of the above being said, the logic behind the strengthening approach does make sense to me and is, as mentioned, consistent with treatment protocols for some forms of tendinopathy. If my PF decided to return at some point it’s a treatment I would consider, but I would like to know a bit more about how it performs relative to a control.
You might also like:
 Army Study: No Difference in Injury Rates Between Traditionally and Minimally Shod Soldiers
Army Study: No Difference in Injury Rates Between Traditionally and Minimally Shod Soldiers
 Study Suggests that Barefoot Running Transition Injuries are Uncommon – What Do You Think?
Study Suggests that Barefoot Running Transition Injuries are Uncommon – What Do You Think?
 Repetitive Overuse Injuries in Runners: Causes and Prevention Strategies
Repetitive Overuse Injuries in Runners: Causes and Prevention Strategies
 Another Study on the Efficacy and Potential Benefits of a Retraining Protocol to Increase Running Cadence
Another Study on the Efficacy and Potential Benefits of a Retraining Protocol to Increase Running Cadence















This is interesting. I’ve dealt with severe PF and found strengthening and foam rolling my calves to be the best way to get rid of it. Stretching didn’t seem to anything and didn’t provide relief.
I initially had PF that was so bad I couldn’t walk and was forced to rest. But I had another, less severe bout four month later and use foam rolling and continued strengthening to get rid of it in a few days.
Can anyone further explain the ‘windlass-mechanism’ referred to in the strengthening exercise? And precisely how the raising of the toes during the exercise changes it? Cheers
This explains it well: link to runresearchjunkie.com
When I had a bout of Planter Fasciitis which plagued me for half a year what seemed to cure it was when I upped my mileage, running lots more miles, but perhaps crucially most of these miles were at an very easy effort.
I have had a couple of minor flair ups since that lasted for a day or two but these never turned anything, I just kept training through these boughts and the problemed disappeared. Again using lots of very easy recovery runs seemed to enable my body to heal quickly.
I think getting the body in place that it heals efficiently is the key to PF, much like other injuries. Specific treatments to the area that ignore the rest of the body and lifestyle will not achieve the best results. Eat well, sleep well, be mindful and come down from life stressors quickly to a relaxed positive state. Exercise regularily but predominantly in a zone of low physical and mental stress, and use high intensity/high stress sessions sparingly.
In a hormone level one could view at very simplistic level as balancing Growth hormone vs Cortisol. Too much of the later and the body will steadily breakdown and injuries will appear first in the weakest link in the chain. The whole chain may well be weakened too and ready to break.
To recovery from this weakened state you need to keep Cortisol levels in check and make sure the body has time and rest to allow the Growth hormones to come an do they job in signally tissue repair.
This is one of my very first videos. Very popular and helpful for treating and working on feet issues like the plantar fasciitis, turf toe or morons…
Check this out, hope it helps
link to youtube.com
Exercises are the only way you can overcome repetitive strain injuries. No amount of pain medication, braces, cortisone shots, etc will give you a permanent fix.
I’ve been battling a particularly nasty case of plantar fascitis lately and as a physician I see my fair share of cases. I’ve had it in the past and it’s been a fickle beast that comes and goes without much to explain what helps or doesn’t help. Mine was so bad that I injected my fascia with bupivicaine before a recent half marathon because as we all know, running was not an option. Did manage a PR so that made the post race pain that much more bearable.
I do believe that the -itis in fascitis is a misnomer and should be changed to fasciosis since the true pathology is not inflammatory but rather due to disorganized collagen and fibrinogen response to chronic stress. I do not believe that NSAID therapy should be utilized because it interferes with the normal healing pathway. Tylenol is ok for pain relief as it will not interfere with the normal healing inflammatory cascade.
As for treatment, there is data to support a vast number of therapies including but not limited to: stretching, strengthening, resection/release, dry needling, corticosteroid injection, extracorporeal shock wave therapy (low or high dose), Tenex high frequency ultrasound, whole blood injection, platelet rich plasma injection, and even, get this, radiation therapy (3 grays of radiation to the heel? No thank you). Most post treatment regimens incorporate at least 6 weeks of rest before slow return to activity so it is tough to figure out which therapy is the curative one, the intervention or the rest. Personally, I don’t think corticosteroids work because of the steroid but rather because of the needling before the steroid, but the steroid provides some relief due to decrease in compression on the nerve. If I had my pick I would go with platelet rich plasma or just dry needling as both utilize the body’s own pathway of healing, ramped up by introducing the blood’s own hormonal factors. Till then, I’m in a boot recovering from my PR and will try conventional non invasive therapy for four weeks.
Pete, I’ve been battling on going low level plantars fasciitis. I’d like to try wearing zero drop shoes like you recommended in your post about how you overcame PF. I’m looking for a casual pair of sneakers I can wear around (not for running) and nothing with too many zany colors that I can also wear at work. Any suggestions for a casual pair of zero drop sneakers?
You might look at something like the Altra Instinct Everyday. Altra may also have a few color options of the regular Instinct that aren’t too crazy. You could also check out the Merrell Bare Access.
I fought with Plantar for a year, trying everything, and then I stopped wearing flip-flops around the house and around town. It disappeared.
This is fantastic information, thank you! I have heel spurs, so it’s always good to have more information about what I can do to reduce the pain. Thanks again:)
Melissa
(Hi Pete: Sorry to add to an old post, but this was the last time you discussed PF.)
A couple years ago I got tired of my more-frequent-than-not PF issues, and was also tired of hearing my friends whine about theirs (as I whined back in sympathy).
We were all focused on discussing the many available (and sometimes conflicting) forms of treatment, with the cause being some nebulous concept of “over-use” or “over-training” or simply “It just sorta started happening”.
I decided we needed to stop the cycle, and focus on identifying and eliminating causes of PF, and I was successful!
Not for everyone, but for my friends who shared my preference for a forefoot strike.
The main problem appeared to be with the strike itself (rather than the push). The one thing we all had in common, as we all trained to get faster, was that we were striking harder.
Which is only expected, right? Perhaps, but some of us (including myself) were extending our feet rather close to lockout, and we were jamming the ball of the foot into the ground, which transmits a sudden, sharp pulse to the PF.
The rest found themselves tightening the calf before impact (in anticipation of springing away).
I think both groups were doing the same thing (calf tightening), but with varying ankle position. Given the strong calves common to forefoot-strike runners, that’s sure to put lots of force on the PF at the time of impact.
When we were free of PF, we tried training on softer surfaces (sports fields and padded tracks), which helped. Unfortunately, all of the races we were training for were on roads.
A couple folks got Hokas, but didn’t like the perceived reduction in stability and the loss of feel for the road. (The mid-sole strikers who tried Hokas tended to love them.)
Clearly, we needed to let the foot “meet” the ground more gently, though we had no idea what that really meant, in practice.
We tried lots of ideas, the vast majority of which were either ineffective or foolish. The best we found was using a higher cadence, which seemed to help, but only a little.
Eventually I realized something quite simple: If the road was hard, it meant that our feet had to become “softer”.
That’s what a higher cadence was giving us, but it was a stop-gap measure, an aid, not the complete solution.
I was thinking about foot mechanics when I came up with a different approach: If the forefoot was striking too hard, why not delay the impact of the ball of the foot, and increase the duration of the initial contact? Go from a single contact point to a moving one, spreading the impact out in both area and time. So, I wanted to make initial, gentle contact with parts of the forefoot other than the ball of the foot, which is the definition of supination.
Well, being a fan of America’s Next Top Model (go figure), I instantly remembered how the models tumbled while learning the “Runway Walk”, where each foot crosses over the center line to massively increase hip pivot and sway. That severe line-crossing gait was massive supination (or a twisted ankle if you didn’t, and sometimes even if you did without weight shift).
If models have trouble walking that way, there’s no way we could run like that! Of course not. But we did try gradually bringing our foot strike closer to the center line until we could tell that the outer edge of the foot was making contact just before the ball of the foot.
We initially tried this while running at a relaxed pace (jogging) with a slightly elevated cadence, to minimize overall impact.
Generally, it was enough to try to run on a road or parking lot paint line to get slight but clearly detectable supination.
Then we gradually widened our gait back toward our customary widths while trying to retain that same softer feeling when making contact. Basically, we learned to roll our ankles slightly outward just before impact.
Of course, we promptly reverted to our old ball of the foot contact, but when this happened, we’d do a few steps of “model running” then try again. We made this part of our form check habits.
Then a day came we realized we had gone nearly 3 months without anyone in our group of forefoot-strikers whining about PF.
And none of us were overdoing our supenation, with no significant wear on the outside of our shoe soles.
I’m now nearly two years without any PF issues. The thing is, with my lifetime of long skinny flat feet, I’ve often had PF issues of one kind or another.
I’ve also come to believe that the supenation was a means to an end, more of a trick than a fix. What I believe has actually happened was that our bodies refused to slam the smaller foot bones into the ground, and relaxed the calf a bit before impact, and we in turn learned to better “catch” the post-impact energy with our calves.
I have no idea how to directly share this “calf catch” behavior: “Model running” seems to be an effective way to access that result.
During the past two years I’ve occasionally shared this with others, such as: “Well, when your PF heals, try running gently on a painted line, and see how that feels on your feet. If it feels better, then make your regular gait feel the same way.”
So far, I’ve gotten zero reports concerning any harm from trying this technique (though many quit because it felt “weird”), and over 50% of those giving it real try said they found at least some benefit from it.
Yes, that’s only anecdotal evidence, and possibly contains some Placebo Effect, but it’s what I have. And those folks did it on their own, without supervision, where our initial group worked together, observing each other and sharing perceptions.
My online searches yielded absolutely nothing about using slight supination to “soften” the forefoot strike for road runners. Nor did I find anything about slightly relaxing the calf before impact (less than full tension) to reduce PF injuries.
I’ve since changed the name from “model running” to “centered strike check” (less to explain), but the meaning is the same.
Did I just discover this? Or am I simply failing to use correct terminology in my searches?
What I’d really like to know is why so many of the forefoot strikers I know, including myself, strike harder when they try to go faster. It’s simply not needed!
Thanks for sharing your story Bob. Your fix sounds somewhat like the advice that I think Chi running uses to relax the ankle when running, to basically shut off the calf and let the foot dangle from the shin prior to contact. I think a lot of people have a perception of forefoot striking that is like the way a ballet dancer runs with toes really pointed and this results in hitting the ground too hard with too much plantarflexion. Glad you found a way through PF!
Usually you should not have to stretch the bottom of the foot musculature because most modern day footwear stretches it too much. This is why you should stretch the intrinsic extensors of the foot. Bring the toes down so the foot flexors can fire properly. Also, you want to stretch the toes away from each other so the abductor hallucis can fire properly and supply the plantar fascia with blood. Abductor hallucis is also responsible for supporting the arch. You need to stretch the calf muscle because most shoes today have heel elevation, which chronically shortens the calf muscle.
After your foot bones are in their proper position, the muscles are strong enough to support the foot without too much conditioning. Every find it interesting that people that have never worn shoes in their life never develop plantar fasciitis?
William Prowse
http://www.pfsurvivalguide.com