
Ryan Hall – 2010 Boston Marathon
This is a guest post by Dr. Jeff Moreno, DPT
A common observation in the world of running is the runner that overstrides. I think whether you are in the world of research, or treating runners full-time in a clinical setting, we can all agree that overstriding is suboptimal. We all understand the potential physical implications of this suboptimal running form, and its affect on running economy. What is currently up for discussion is the root cause of overstriding and other less than desirable running forms.
Injury rate in runners has been reported to be as high as 80% in a given year. This is excessive and significant enough to warrant research funding from private and federal organizations. This funding has, and is, allowing for more and more research to be done in the areas of shoe design, foot strike patterns, barefoot running, stride frequency, and understanding the etiology of common lower extremity pathologies found in our runners. We have already learned invaluable information regarding stride length, stride rate, shoes, ground reaction forces (GRF’s), and the effects of biofeedback on running form. The research has provided clinicians with new approaches to treatment that have been easily applied to our runners with some success in reducing pain and allowing for a return to running. However, are we still missing the bigger picture, and if so what next?
My purpose for writing this article is to describe what I am seeing clinically as a physical therapist on a daily basis as I treat runners. The focus of this post is to not only discuss what is being researched currently or what the latest studies tell us, but to give you a clinical perspective that may help us start bridging the gap between the research lab, the clinic, and more importantly on the track/road. With that said, I hope that this will initiate conversation and interest, and that it leads us to look at suboptimal running form and more importantly poor movement patterns and muscular imbalances as part of a greater dysfunction.
If you are still reading, I am writing to you, the researcher and clinician, studying and treating runners on a regular basis. Since you frequently work with these athletes, I am going to assume that you have a background education in biomechanics and analytical anatomy. My only other request is that you have an open mind, and allow yourself to think outside the parameters of what we know the current research in running has shown us.
So with that said, when observing and assessing a runner at any level, I look first at very basic and simple fundamental movements that assess how the running athlete’s brain represents movement from point “A” to point “B”. I am not going to talk about my specific assessment; however, it is important to understand that when I am assessing and/or treating a runner I am really looking at the specific subconscious and involuntary movement that is produced by the brain. The last thing that I do is put them on the table, and this is only to confirm clinically what I saw dynamically during their movement tests and while running. After I have assessed how their brain represents movement, I look at the runner’s ability to resist/control the affects of gravity and then overcome gravity over distance, time, and desired speed. The ability to control and overcome gravity during running requires very specific coordinated patterns of movement with specific timing. Frans Bosch and Ronald Klomp in their book, Running: Biomechanics & Exercises Physiology In Practice, describe running as being cyclical in nature. As stated by Bosch and Klomp (2005), “This means that a previous movement will have a great influence on the following movement. The motor system needs information obtained from the previous step [swing] before taking the next step [initial contact/loading]. The body is geared to copy patterns of motion continuously [good or bad]” (p. 132). In other words, the action of the swing leg will dictate that of the stance leg (and vise versa). Both motions are unconsciously and involuntarily related (e.g., motor program, Central Pattern Generator; optimal or suboptimal). Therefore, running has been described as a contralateral pattern like that of crawling/walking with the opposite arm and leg moving together in a coordinated fashion to ultimately produce forward motion.
For those of you treating runners, the depth and breadth of your understanding of normal movement and gait needs to be very high in order to truly understand abnormal movement/gait. The more you observe the walking/running gait the more you start to pick up the subtleties of gait. The Frans Bosch “method”, recently summed up by Jeff Cubos, DC, on effective coaching and performance therapy, suggested one should consider the following:
-Know what you see
-Know what you don’t see
-Know why you don’t see what you don’t see
-Know how to best get what you want to see
– …so that you can see it consistently
Therefore, looking at the walking and running gait globally as a series of optimal or less than optimal patterns, I believe, is extremely important and often overlooked during gait analysis. Current research and our understanding of causative biomechanics has given us specific invaluable information on less than optimal movement during initial contact and loading phase during running (e.g., hip adduction, pelvic drop, tibial rotations etc…). However, if running is truly cyclical and dependent on the phase prior, then the swing phase just prior to initial contact and the contralateral stance phase is just as important as the loading phase. If this is so, which I believe to be true, why then is all our current research focused primarily on one small piece of the pattern? Yes, I understand that loading rates and higher impact peaks due to suboptimal loading can be a cause for some of our most common running injuries, but I think it is time to move on and step outside the box (speaking to the researcher). I see these stance phase injuries as a product of a greater dysfunction that cannot be explained only by what is happening at the time of the visual dysfunction, but as a byproduct of a poor global pattern. This has allowed me to assess runners through a different lens and not only treat the products of a poor loading phase (e.g., weak glutes), but also treat the patterns of movement that led to the poor timing and motor control of the glute during stance phase.
Everybody, I believe, has a unique kinetic signature during running that can make an individual’s gait unique to themselves. However, there are also very important coordinated patterns of movement that must occur during the running gait. I come from the world of distance running, and like all distance runners, I think sprinters are a special breed! With that said, some of the best minds in coaching/running come from the world of sprinting, and if you have spent any time on the track and have listened to and read what these great coaches (Dan Pfaff, Tom Tellez, Irving “Boo” Schexnayder, Loren Segrave, Ralph Mann, etc…) have to say you would realize quickly that they spend a significant amount of time on developing a highly skillful athlete.
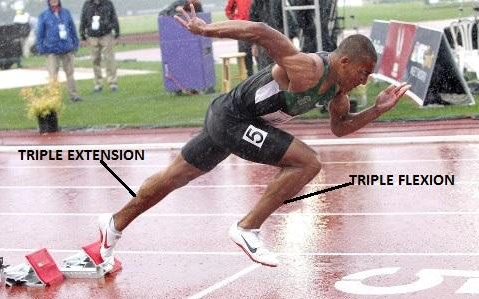 When looking at sprinters versus distance runners, I see very defined patterns of motion in sprinters that are much more consistent across individuals than in distance runners. Sprinters have an amazing ability, due to training and biomechanical/kinesiological demands, to achieve triple flexion during swing (hip flexion/abduction/external rotation, knee flexion, ankle dorsiflexion) and triple extension during propulsion (hip extension/internal rotation, knee extension, ankle plantar flexion). The flexion and extension patterns in runners and sprinters are always cyclical and require high levels of coordination and timing. These triple flexion and extension patterns are obviously accentuated in the sprinter versus the distance runner as seen above; however, the pattern should always be expressed in any runner regardless of speed or talent.
When looking at sprinters versus distance runners, I see very defined patterns of motion in sprinters that are much more consistent across individuals than in distance runners. Sprinters have an amazing ability, due to training and biomechanical/kinesiological demands, to achieve triple flexion during swing (hip flexion/abduction/external rotation, knee flexion, ankle dorsiflexion) and triple extension during propulsion (hip extension/internal rotation, knee extension, ankle plantar flexion). The flexion and extension patterns in runners and sprinters are always cyclical and require high levels of coordination and timing. These triple flexion and extension patterns are obviously accentuated in the sprinter versus the distance runner as seen above; however, the pattern should always be expressed in any runner regardless of speed or talent.
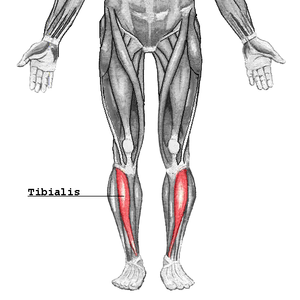
Now, understanding that running is highly coordinated and cyclical, I want to present what I am seeing clinically. I have had the privilege and opportunity to treat runners of all levels from Olympians to recreational runners. Working with these runners, whether injured or not, I am seeing very distinct patterns regardless of the level of ability and talent. Currently, in the world of running if you ask anybody regularly treating runners at any level what is the most important motion that a runner should possess, they will most likely say hip extension. I believe that hip extension is extremely valuable and needed to coordinate movement appropriately during running; however, in the clinic I only truly find a significant loss of monoarticular (iliopsoas) hip extension necessary to run approximately 25% of the time. Most runners, I have come to believe, have the ability to extend their hips, whether they take advantage of their available hip extension is another story. (By the way, most of the force that we produce whether running or sprinting occurs from initial contact to mid-stance at which point force decreases rapidly – a little off topic but something to think about). With that said, I do often find a significant restriction of the biarticular hip muscle rectus femoris. Does the short and/or stiff biarticular hip flexor and knee extensor (rectus femoris) result from overuse? Absolutely! I believe significant overuse of this two-joint hip flexor, along with the TFL (tensor fasciae latae), is resulting from the poor ability to control gravity and coordinate movement. These two muscles are primarily active during mid swing and at the end of swing to mid-stance. Why is this occurring? I will try to explain.
 What I am seeing clinically is not poor hip extension, but just the opposite, poor hip flexion, and the ability to coordinate hip flexion appropriately with hip abduction and external rotation (triple flexion) at the same time during all movement, not just running. So, if I had to group the most common pattern of impairments that I am seeing in my distance runners, it would be as follows: swayback posture, thoracic kyphosis (stiff), forward head, poor abdominal control/coordination, poor hip stability, long and weak iliopsoas, stiff rectus femoris/TFL, knee hyperextension, relative plantar flexion in standing, forefoot varus, and poor intrinsic foot strength (see picture for example). When running, these impairments listed above often result in poor outcomes like overstriding, abductory twists (tibial rotations/whips), crossover effects, pelvic asymmetries, femoral rotations, posterior center of mass (COM), lower extremity pendulum effects, etc. I see this postural dysfunction in all levels of athletes from elite to recreational. These same runners, when asked to perform simple fundamental patterns of movement like a squat (i.e., triple flexion), single leg balance, step down, quadruped rock back, etc… struggle and often can’t coordinate very basic patterns of movement that are necessary for walking let alone running. How many of your runners when squatting or single leg squatting can easily disassociate their hip from their pelvis/spine and move their hip independently with ease like a highly skilled runner would? These athletes will express the same poor pattern of limited hip flexion and excess hip adduction and internal rotation regardless of the movement asked to be performed. Now, given that the human body is efficient and always moves first toward the path of least resistance, the body chooses these patterns of movement subconsciously/involuntary to be more efficient. This has forced me to try and answer what is driving these suboptimal movement patterns that have become hardwired motor programs in our runners?
What I am seeing clinically is not poor hip extension, but just the opposite, poor hip flexion, and the ability to coordinate hip flexion appropriately with hip abduction and external rotation (triple flexion) at the same time during all movement, not just running. So, if I had to group the most common pattern of impairments that I am seeing in my distance runners, it would be as follows: swayback posture, thoracic kyphosis (stiff), forward head, poor abdominal control/coordination, poor hip stability, long and weak iliopsoas, stiff rectus femoris/TFL, knee hyperextension, relative plantar flexion in standing, forefoot varus, and poor intrinsic foot strength (see picture for example). When running, these impairments listed above often result in poor outcomes like overstriding, abductory twists (tibial rotations/whips), crossover effects, pelvic asymmetries, femoral rotations, posterior center of mass (COM), lower extremity pendulum effects, etc. I see this postural dysfunction in all levels of athletes from elite to recreational. These same runners, when asked to perform simple fundamental patterns of movement like a squat (i.e., triple flexion), single leg balance, step down, quadruped rock back, etc… struggle and often can’t coordinate very basic patterns of movement that are necessary for walking let alone running. How many of your runners when squatting or single leg squatting can easily disassociate their hip from their pelvis/spine and move their hip independently with ease like a highly skilled runner would? These athletes will express the same poor pattern of limited hip flexion and excess hip adduction and internal rotation regardless of the movement asked to be performed. Now, given that the human body is efficient and always moves first toward the path of least resistance, the body chooses these patterns of movement subconsciously/involuntary to be more efficient. This has forced me to try and answer what is driving these suboptimal movement patterns that have become hardwired motor programs in our runners?
 A good example of this dysfunctional pattern is the runner that was described above with swayback posture and a long and weak iliopsoas and stiff rectus femoris. This runner will have a poor ability to triple flex due to insufficient passive and active kinetic energy from the anterior hip muscles (poor elastic recoil) resulting in an altered triple flexion pattern. The weak and long iliopsoas and dominant biarticular rectus femoris muscle will prevent sufficient hip flexion in swing, and will most often result in excess knee extension during the end of the swing phase to advance the lower extremity (see picture above). Therefore, we cannot expect the contralateral lower extremity to function in a coordinated fashion due to the cyclical nature of the running gait. The pattern becomes altered and instead of hip flexion/abduction/external rotation, knee flexion, and ankle dorsiflexion (triple flexion pattern), the runner displays excess knee extension with hip adduction at the end of swing to advance the lower extremity (rectus femoris/TFL dominance). Fifty percent of my patients will complain of knee pain with this type of gait, but you can imagine the other potential biomechanical implications during the loading phase that can be produced due to this poor coordination of gait.
A good example of this dysfunctional pattern is the runner that was described above with swayback posture and a long and weak iliopsoas and stiff rectus femoris. This runner will have a poor ability to triple flex due to insufficient passive and active kinetic energy from the anterior hip muscles (poor elastic recoil) resulting in an altered triple flexion pattern. The weak and long iliopsoas and dominant biarticular rectus femoris muscle will prevent sufficient hip flexion in swing, and will most often result in excess knee extension during the end of the swing phase to advance the lower extremity (see picture above). Therefore, we cannot expect the contralateral lower extremity to function in a coordinated fashion due to the cyclical nature of the running gait. The pattern becomes altered and instead of hip flexion/abduction/external rotation, knee flexion, and ankle dorsiflexion (triple flexion pattern), the runner displays excess knee extension with hip adduction at the end of swing to advance the lower extremity (rectus femoris/TFL dominance). Fifty percent of my patients will complain of knee pain with this type of gait, but you can imagine the other potential biomechanical implications during the loading phase that can be produced due to this poor coordination of gait.
If you are a skeptic, test this for yourself. Go outside right now and run with high knees or up a steep hill (to accentuate hip flexion) and ask yourself what happened to your knee during mid to late swing prior to initial contact, as well as, the reactivity of your hamstring prior to initial contact. Now, go run while limiting hip flexion, and ask yourself what happens to your knee motion at the end of swing and during initial contact. You will have noticed that when accentuating hip flexion it is almost impossible to create excess knee extension during the end of swing to initial contact; however, when limiting hip flexion you will have noticed immediate excess knee extension and possible overstriding in order to advance the lower extremity.  What you just performed was outside of your voluntary control and part of a global pattern; one optimal verses the other suboptimal. Remember, these two patterns that you just performed are global and coordinated (see pictures above and below of less than optimal versus optimal triple flexion respectively)! The limited hip flexion with subsequent overuse of the rectus femoris to advance the lower extremity can inevitably result in the base of support (BOS) being significantly in front of the COM, leading to larger loading rates and impact peaks. I am seeing these abnormal patterns of movement expressed clinically regardless of strike pattern, shoe type, speed, flexibility, strength, and even in the presence of a stable trunk. I think all of us treating runners on a daily basis would agree that it is not all about the “shoe”, but more what the running athlete puts into the shoe!
What you just performed was outside of your voluntary control and part of a global pattern; one optimal verses the other suboptimal. Remember, these two patterns that you just performed are global and coordinated (see pictures above and below of less than optimal versus optimal triple flexion respectively)! The limited hip flexion with subsequent overuse of the rectus femoris to advance the lower extremity can inevitably result in the base of support (BOS) being significantly in front of the COM, leading to larger loading rates and impact peaks. I am seeing these abnormal patterns of movement expressed clinically regardless of strike pattern, shoe type, speed, flexibility, strength, and even in the presence of a stable trunk. I think all of us treating runners on a daily basis would agree that it is not all about the “shoe”, but more what the running athlete puts into the shoe!
As a side note, to those clinicians that have spent time in a neurological rehabilitation setting treating stroke or traumatic brain injury patients, you will probably recognize that pattern of gait when limiting hip flexion. These patients express significant limitation in active hip flexion (depending on the affected area of the brain), which ultimately produces knee hyperextension, ankle plantar flexion, and subsequent circumduction of the lower extremity to advance limb forward during gait. This is due to a cerebral vascular accident or traumatic brain injury resulting in hemiparesis. I am not saying that these runners have had a CVA or TBI, but from a neuromuscular perspective they demonstrate similar patterns of movement globally speaking (you neurological buffs, something to think about).
I first wrote about this pattern two years ago and there was very little interest within the running community, but a recent study in the Journal of Biomechanics by Noehren’s group out of the University of Kentucky has been published which may shed some light on the possible importance of hip flexion in reducing loading rates and impact peaks during running. Many studies have been published looking at forces and loading rates contributing to overuse injuries in runners. The goal of this recent study was to look at different variables that may predict magnitude of impact peak and loading rates, as well as how different knee and hip muscles during swing affects these loading forces. The results suggested increased hip flexor activity and higher positioned thigh during mid swing decreases velocity of the leg at landing leading to smaller forces at impact (Thank You Noehren’s group for studying something other than differences in shod vs unshod runners!).
If we look at this from a biomechanical and kinesiological perspective, what effect does hip flexion during the swing phase have on muscle activation of the hip extensors and knee flexors prior to contact? Understanding that running is cyclical, what happens during swing can and does affect loading phase. Preparatory muscle activity during mid to late swing in recent studies has been shown to be important in the role of foot-ground contact. This preparatory muscle activation enhances the control of muscles during the subsequent loading phase, leading to better lower extremity muscular stiffness. This is accomplished by the facilitation of the gluteus maximus and hamstrings (and others); due to proper triple flexion during swing, to prepare the lower extremity for ground contact. Clinically, I am seeing a lack of passive and active kinetic energy during swing hip flexion at a runner’s preferred speed. I believe this is limiting the preparatory gluteus maximus and hamstring activation ultimately resulting in excess knee extension during late swing and the potential for higher forces at impact. To all those in the research lab, what would be interesting is to look back through all of your past data amassed on those fancy treadmills and force plates, and see if there is a correlation between those that have less hip flexion and more knee extension during end of swing/initial contact in those that overstride and those that don’t at a constant speed.
Now to the question, why is this combo of swayback posture, thoracic kyphosis (stiff), forward head, poor abdominal control/coordination, poor hip stability, long and weak iliopsoas, stiff rectus femoris/TFL, knee hyperextension, relative plantar flexion in standing, forefoot varus, poor intrinsic foot strength, and the subsequent lack of dissociated hip flexion so common? Well, let me tell you, this leads me to my final observation and area of interest. Culturally, we are very different in the US versus other non-industrialized nations. As a culture, the United States and other western cultures have seen a significant increase in postural related dysfunctions from the head to toe. We, as a society have lost our ability to resist the affects of gravity in all weight bearing activities, let alone running with 2.5 to 3.0 times body weight while on one leg. I have defined this as the gravity intolerant runner. Knowing that we are culturally intolerant to the forces of gravity due to pervasive inactivity and prolonged sitting; I believe that this evolution of our structure and function has resulted in suboptimal patterns of movement during running. Those distinct patterns that are seen in our running patients/clients of swayback posture, posterior COM, stiff rectus/TFL, knee hyperextension, ankle plantar flexion, and forefoot varus position, I believe, are a result of our cultural intolerance to gravity. As a result of this pervasive global intolerance to gravity, the running athlete’s perception of normal posture has been altered resulting in significant neuro-musculoskeletal imbalances leading to many of the impairments commonly related to most running injuries. As a culture we have developed talent in the absence of skilled coordinated movement.
How do we overcome this? Let’s get our runners, coaches, and health professionals to understand that developing talent starts with developing the skill of movement and postural tolerance to gravity. Let’s take our knowledge of causative biomechanics and kinesiology and apply it to correcting altered patterns of movement that are contributing to all the impairments that we see in our every day runners. More importantly if we really want to reduce running-related injuries in the future let’s first start by asking our youth to go outside and run, jump, climb, push, pull, roll, and even fall to naturally increase postural tolerance to gravity!
My challenge to all those do running-related research and those treating runners are:
1. Look globally!
2. Understand that to run efficiently the runner had better resist/control and overcome gravity well!
3. Understand that running is a series of coordinated patterns of movement that require proper timing.
4. Look at running cyclically and know that what is happening in stance is dictated by what the swing leg is doing and vise versa.
5. The human body is highly adaptable which means that the human body can unfortunately be efficiently inefficient!
6. Swing phase is just as important (IN MY MIND MORE IMPORTANT), than stance phase when it comes to running related injuries.
7. How much are you looking at swing phase influencing what happens at stance phase with your injured runners? Are you treating patterns of movement or just parts of the pattern (e.g., pelvic drop, weak glutes)?
8. Can we please start bridging the gap between the track/road and the research lab. In order for this to occur that would require some of our brightest minds in the lab to start speaking with the coaches primarily working with these athletes (In A Perfect World).
9. Can we please move on from the shod versus unshod debate, PLEASE!!! There is so much more going on globally with the running athlete than just what is happening at the foot/ground interface.
Let’s start discussing!
Jeff Moreno, DPT, OCS
Precision Sports Performance Running
References
1. Bosch, F., Klomp, R. (2005). Running: Biomechanics & Exercise Physiology Applied in Practice. Philadelphia, PA: Elsevier.
2. Chumanov, E., Wille, C., Michalski, M., Heiderscheit, B. (2012). Changes in muscle activation patterns when running step rate is increased. Gait & Posture, 231-235.
3. Dietz, V. (2002). Review: Proprioception and Locomotor Disorders. Neuroscience, 3, 781-790.
4. Frank, C., Kobesova, A., Kolar, P. (2013). Dynamic Neuromuscular Stabilization & Sports Rehabilitation. International Journal of Sports Physical Therapy, 8 (1), 62-73.
5. Kyrolainen, H., Belli, A., Komi, PV. (2001) Biomechanical factors affecting running economy. Medicine Science Sports Exercise, 33(8), 1330–1337.
6. Novacheck, T. Biomchanics of Running. (1998) Gait & Posture, 7, 77-95.
7. Saunders, P., Pyne, D., Telford, R., Hawley, J. (2004). Factors affecting running economy in Trained Distance Runners. Sports Medicine, 34 (7), 465-485.
8. Schmitz, A., Pohl, M., Woods, K., Noehren, B. (In Press). Variables during swing associated with decreased impact peak and loading rate in running. Journal of Biomechanics.
9. Weyand, P., Sternlight, D., Bellizzi, M., Wright, S. (2000). Fast top running speeds are achieved with greater ground forces not more rapid leg movements. Journal of Applied Physiology, 89, 1991-1999.
You might also like:
 Is Forefoot Running a “Cure” for Chronic Anterior Compartment Syndrome?
Is Forefoot Running a “Cure” for Chronic Anterior Compartment Syndrome?
 Moses Mosop Bounces on his Forefeet and Floats Through the Air to Win the Chicago Marathon!
Moses Mosop Bounces on his Forefeet and Floats Through the Air to Win the Chicago Marathon!
 More On Running Cadence: Comparative Data from Amby Burfoot and Alex Hutchinson
More On Running Cadence: Comparative Data from Amby Burfoot and Alex Hutchinson
 Running Speed: Human Variability and The Importance of Both Cadence and Stride Length
Running Speed: Human Variability and The Importance of Both Cadence and Stride Length
 Proprioreception: Additional Thoughts on Balance, Stability, and Running from Jay Dicharry
Proprioreception: Additional Thoughts on Balance, Stability, and Running from Jay Dicharry















I love being given another window of perspective for looking at runners, athletes and their subsequent injuries. I agree with a lot of this post and I am seeing these postural dysfunctions at all levels as well. Integrating dysfunctional gait patterns, poor movement patterns and postural/respiratory dysfunction is going to be the next big wave in treating runners and their injuries. Don’t get stuck looking at just one thing.
Thanks for the comment Adam!
“If you are still reading, I am writing to you, the researcher and clinician, studying and treating runners on a regular basis.”
Well, golly, I guess I’m just too dumb to understand all the big words you guys use. Guess I’ll just go out for a run, like this: (I’m the one on the right) /Users/michaelmayhew/Desktop/Screen shot 2013-12-05 at 2.18.54 PM.png
OK, guess that screenshot didn’t show up. Feel free to delete the comment, but I think the picture demonstrated good form.
Michael,
Jeff is a PT and the point of his article was to get people who work in gait clinics to look at running gait in a different way. He’s not trying to belittle anyone, and I can tell you I frequently get comments asking me to translate some of the science I put into my own posts.
Pete
I am pretty sure I am a good example of being gravity intolerant with hip flexion issues with Pete documenting me early in November with many real useful commentators providing analysis, a lot along the lines of this article. I do not have injury issues despite my gravity issues! link to runblogger.com. This article is excellent in providing some good science and societal reasons as well. Now that the diagnosis is given what is the prescription?
Sam – just added your video embeds back in after seeing your comment, so they are back up now. Dealing with YouTube is going to be achore, one post at a time!
Next time you run try the trick Jeff mentions about lifting your knees/flexing thigh during forward swing. Curious to see what it does for you.
I enjoyed this article! Because, unlike most of the articles on this subject, I can tell that you have put some time into actually working one-on-one over a treatment table with runners/athletes in a clinical setting.
What also comes through in your writing, is your ability to think, which is a skill that is underutilized in the world of rehab (and prehab!).
Human function is about timing, and sequential strength. And at the end of the day, both are determined by the brain.
In order for a bone to go into a position at a joint, the brain and the muscle have to sense stability in that position(s).
Whenever the brain and the muscle are not willing to cooperate, there will be a tight muscle to prevent the bone from going into the desired position(s)at the joint.
So, yes, the swing leg is just as important to our overall function. Unfortunately, the point at which the lead leg comes in contact with the ground tends to get all of the attention.
In order to have an efficient supination and/or propulsion on one side, *all* of the muscles on the side of the swing leg have to be capable of firing optimally.
If a muscle is not receiving the appropriate input to pull *everything* on the side of the swing leg, it is impossible to have efficient motion of the foot (and everything above it) on the opposite side.
Ultimately, human function always comes back to the same question: Can each and every muscle generate enough internal force to pull, at the right time, in the right plane, and at the right joint?
Whenever the answer comes back as No, you will not have symmetry between the two sides.
To say the same thing in slightly different way, if everything is not moving at the right time on one side of the chain, it will be impossible for everything to move at the right time on the opposite side.
In other words, the swing leg is driving motion into supination on the opposite side. But, in order to drive those motions, the muscles on the opposite side have to be capable of generating enough force to pull everything back home for an explosive propulsion.
That being said, running requires motion of the entire chain. From the environment of the foot, all the way up to the jaw, it’s all equally important to the overall success of the runner/athlete.
Whenever (and wherever!) something is off as it relates to timing, the foot will remain on the ground (much!) too long.
Then, when the brain and muscles can no longer adapt to the demands that are placed upon them, pain and/or an injury will settle in.
I’m not going to go as far as to say that hip extension is overrated in the running space, however, in order to get extension of the thigh at the hip joint, you first have to have motion into extension at the lumbosacral joint and spinal joints. And when you don’t, (which is usually the case), you will have a limitation of the thigh to extend at the hip joint.
To say it another way, that is just one of many reasons why the Thomas Test is a waste of time.
Note: In order for the thigh to extend and/or flex at the hip joint, the starting position of the pelvis also comes into play.
I applaud you for suggesting that the psoas major (and TFL) are most likely weak in the image that showed a runner’s static posture.
However, if you consider what the brain is willing to allow for, I’m betting that improving transverse plane motion of the pelvis/trunk, will change what the image is showing as primarily a sagittal plane adaptation.
In other words, I have to ask, are you really seeing, what you think you are seeing as it relates to a “weak” psoas and/or TFL?
An aside: The rectus femoris is a superficial muscle, and its friends from the same group are deeper, i.e., the quadriceps. Not only that, they also wrap around to attach all along the posterior side of the femur. So, based on their depth, amount of attachment to the femur, and fiber direction, they are much more capable of providing not only more neurological stiffness, but also much more leverage.
So, it’s hard to imagine the rectus femoris, a muscle that is superficial and runs in a straight line, being more important than muscles that are much more equipped to play a bigger role in all three planes of motion in the running gait cycle. Not only at the hip (femur and pelvis), but also the lower leg at the knee joint.
One of the amazing things about the world of rehab (and prehab!) is this notion that if we “strengthen” the core musculature everything will function better.
The reality is, the core musculature is the same as any other muscle and/or group of muscles in the chain, they are all relying on optimal feedback from the brain to pull a joint(s) into a position.
I’m sure you would agree that it’s very difficult to zoom in on what is really happening when assessing the running/walking gait cycle.
There are just to many moving parts to get an accurate assessment of what is actually occurring at each and every joint throughout the chain. Yes, you might get some indications as to a strategy that the runner/athlete is using to get from point A to point B over many miles, but even then, it’s still the next best guess as to what is really occurring.
Rick, thank you for your insightful comments. I appreciate that you really understand that it is the brain that we are really dealing with when treating any athlete. Regarding static posture, gait, and fundamental movement patterns, I believe, is a window into how the athlete represents movement. As a result, the picture of individual standing, will functionally choose their TFL and rectus for hip flexion based on its mechanical advantage in that position. Is it truly weak, I almost don’t care, I am going to treat the dysfunctional pattern and not try to improve isolated muscle function. Treatment was not discussed, but if I give her a fixed point (puntum fixum) Pelvis/Spine for her femur during hip flexion then she will probably demonstrate better function at her psoas. Strength to me is the ability to resist fatigue over time. This starts with optimal coordinated movement. Great post, and I love how you think!
Jeff, this is brilliant!
Thanks for taking the time to put the article together. I’d describe myself as a run coach and sports rehabilitation therapist in equal measure. I completely agree with your comments in terms of the vital importance of assessing with the cyclical nature of running gait in mind, and our industry’s frustrating tendency to focus primarily on stance phase. I constantly find myself trying to explain to runners (non-clinical) that in general terms “the quality of your foot-strike and subsequent stance phase is only as good as your swing mechanics will allow…”
Weak Iliopsoas combined with a swing phase dominated by Rec.Fem./TFL is a pattern I see daily in runners and triathletes. This hip flexor imbalance has been the focus of some good work by Shirley Sahrmann, I believe. It is certainly helped by Iliopsoas strengthening and appropriate cues in terms of gait-retraining to re-establish co-ordination of triple flexion as an important precursor to effective triple extension. I do also find that cueing the hamstrings to become *a little* more active in early swing phase to flex the knee has a positive effect in shortening the lever acting at the hip, potentially reducing required hip flexor torque to achieve adequate hip flexion. This talk of cueing hamstrings is kind of beginning to sound like POSE – I’m not a POSE coach or advocate per se…!
As an aside, I find this thought process to be brilliant in re-educating swing phase in athletes suffering with ITBS – a good example of a pathology where I feel too much emphasis is (in some cases) placed on stance phase biomechanics. We need to assess both stance and swing, particularly looking at muscle imbalances created at the hip by suboptimal swing mechanics.
In terms of lower leg, foot and ankle issues: another common pattern I see is the athlete with inadequate hip flexion in mid-to-late swing phase compensating with increased knee extension prior to initial contact (over striding heavily), then relying on an increased ‘ankle rocker’ to work through stance phase. This comes in lieu of effectively recruiting G.Max driving the limb into triple extension top-down with powerful hip extension (because this lack of hip flexion inhibits pre-loading). Again, when trying to explain this to the ‘every day athlete’ I describe it as ‘running with your ankles, due to not effectively using your hips’. We re-educate the hips, and often lower leg symptoms subside.
Perhaps it’s because 80% of my client base are triathletes, but I do see a significant lack of hip extension in SO many athletes I assess. Many not even close to zero degrees hip extension in a Thomas test. Upon closer inspection, the majority of these athletes are indeed limited into hip extension by Rec.Fem, rather than Iliopsoas, as you say.
“Can we please start bridging the gap between the track/road and the research lab.” – YES!! This is what the running community needs more than anything. There is some great research being produced at the moment. It’s the practical application of this research that makes it worthwhile :)
Thank for the comment James, lots to think about. I also see lots of cases of limited hip extension, but typically ascribed it to the iliopsoas being tight. Definitely need to think more about the RF. Was playing with emphasizing hip flexion in swing today on my run and it is quite a different feeling. Love thought provoking posts and comments like this!
Jeff thanks for this. I too have seen and evaluated 100’s or runners. the posture is critical and for a runner to find “their” pattern it cannot be overcoached. just got back from The Running Event in Austin where we placed well over 100 runners from recreational to Olympians on a motorless treadmill called True Form Runner. the elites get on it and roll….they have it dialed in. those who overstride need a few cues and then they figure it out immediately. Wild to watch. We created a few training videos here spontaneously
link to samsarafitness.com . These were shot w no script on my first experience with this machine. Could be a tool to help runners get better posture and fix their forms. I’ll be in LA in January to teach a course. maybe i’ll get to meet you. Mark
Mark – so does the treadmill not work well if you overstride? That could be an interesting tool. what’s the price tag?
Pete
Mark- I need to go to The Running Event in Austin one of these years. It sounds amazing! I love your website and appreciate people like yourself and Pete who are passionate about developing skillful running athletes. One of these days we will have to all meet and talk anything and everything running.
Mark needs to have another summit in Shepherdstown like we did a few winters ago :)
Mark, that treadmill looks amazing. The videos you made over at samsarafitness are very clear and well done as is the feedback from using the treadmill on form. The idea of doing a short stint on the treadmill before going out to “feel” the sweet spot seems very valid. As Pete asks how much for that wonder?
This all went pretty far over my head!
Same here. If running form is so incredibly complex as this article maintains, what hope does a layman like me have? I might as well give up now and buy a bike.
Steven don’t fear. Any and all movements are complex, however, it is my job and the job of other clinicians and coaches to simplify it, so that you don’t have to think so much. This article was primarily meant to foster discussion between researchers, clinicians, coaches, as well you the athlete, so that we can keep people like yourself training uninterrupted for years to come. Continue to master the skill of running and find someone that you trust if you need help doing that.
Enjoy the Process and Keep Running!
Pete, Jeff, Sam,
the commercial grade T-mill is a bit over 5k. nothing to ever wear out w stainless steel bearings. product just coming out. more soon. Pete would love you to do some filming of runners on this and compare to regular T-mill or ground. owners are close to you in CT. They run a vineyard so can bring wine too :) Mark
Where in CT? I’ll be down there right after Xmas
I still think it works better being unshod when one does exercises to increase one’s resistance to gravity, as he describes it. Good triple flexion comes not as a result of trying to do that, it’s a by-product of everything working properly. Get yourself balanced in a one-legged stance, have good, neutral posture, and perhaps do some one-up kind of exercises, and you’ll be training your system to operated optimally. Dancing also helps. Stiff, weird movements on the dance floor equal stiff motion in general. There’s a video on Youtube of Gebrselassie doing an easy run on the beach. Before he runs, he does a little warm-up “dance” to get himself loose, I guess. There’s also that video of the Australian hurdler girl doing her little sexy dance routine before a race. All of these things help coordination and add to the sense of play and flow that many Americans may be missing in their movement patterns.
I meant the 100-up exercise, but perhaps a little more sexy and looser than like the dude who came up with it did it.
link to 100up.info
Thanks for the post Jeff and Pete.
Its nice to see the importance of hip flex or hip flexor torque discussed. Both Ralph Mann and David Winter stressed this in their research. Here is a post I wrote talking a bit about their work
link to thebodymechanic.ca
More recently Anthony Schache, Time Dorn and Sam Hamner have all done great work on the kinetics of running. They certainly focused on the role of the hips during swing. Tim’s site is here with great full text articles link to timzone.net
Tim’s counter intuitive finding that the swing legs extensor torque at the end of swing creates hip extension accleration in the opposite leg at toe off is very interesting (e.g via Dynamic Coupling)
It seems you are basically suggesting that good hip flexion decreases overstriding and thus we have less impact/collision. I posed a related question to Anthony Schache last year and he sent me two graphs showing hip flexion angle as running speed increased. What they showed was as hip flexion increased there was not less hip flexion at footstrike (I don’t know about knee angle)and in one subject there was greater hip flexion at footstrike (i.e an overstride)even as hip flexion increased.
I think your question about researchers going through their data would be great to see. I may even play with my 3d kinematic system and see what we can find. Email me if you have ideas
My more critical questions about your post are (sorry :) ):
1. I don’t think you can look at a runner and see their “active and passive” contributions to joint torque. I don’t see this as a valid assessment tool
2. I wish that we would stop getting hung up on these antiquated views of Kendall and Sahrmann “faulty” posture. Static posture has a poor link to dynamic function and is certainly not related to pain.
3. I don’t think we have any valid method of looking at someone run and saying that their psoas is not contributing to hip flexion and its their TFL or RecFem. You just can’t look at kinematics and surmise what the muscles are doing to create that movement. If you have some validated ways I would love to change my mind.
Great and interesting post.
Greg
Greg-thank you for posting and bringing to my attention the great work that Anthony Schache and Tim Dorn are doing right now in the world of gait. Tim is currently at Stanford University which is only a 45 minute drive from Santa Cruz, Ca where I live. Small World!
As you know running is extremely complex and requires highly coordinated patterns of movement with specific timing. Understanding human development and normal gait helps to give us a baseline understanding in these complex patterns of movement, which allows us to look a patients/clients with greater specificity. Unfortunately, most clinicians and coaches don’t have access to 3D motion capture software and treadmills with force plates. Therefore, due to the confines of insurance, financial resources, and time we use our understanding of normal movement and the neuro-musculoskeletal system to hypothesize “Why”, for example, a runner is developing 5 stress Fx’s in the right tibia in a two year span (NCAA Division I collegiate runner of mine).
Let me try and answer your questions:
1. I don’t think you can look at a runner and see their “active and passive” contributions to joint torque. I don’t see this as a valid assessment tool.
I agree with you that it is impossible to know objectively what specific active and passive contributions to joint torque are during specific phases of gait. However, if I see runner that purely runs on his/her forefoot with and early heel off prior to mid-stance, I can hypothesize that this may result in poor ipsilateral hip extension due to the dominance of the plantar flexors (pseudo hip/gluts) and contralateral hip flexion during swing. I am also going to question their ability to generate torque actively and passively at their hip. I will also ask myself if this is increasing the joint torque at their ankle, possibly explaining their history of achilles tendinopathy, MTSS, metatarsalgia etc… As you know, we use our understanding of current research, and what we see in the clinic, through our assessment, to bolster our clinical reasoning process.
3. I don’t think we have any valid method of looking at someone run and saying that their psoas is not contributing to hip flexion and it’s their TFL or RecFem. You just can’t look at kinematics and surmise what the muscles are doing to create that movement. If you have some validated ways I would love to change my mind.
The psoas muscle and all the other muscles that synergistically produce hip flexion are always going to contribute to forward motion of the leg. I am definitely not saying that the psoas muscle is completely off. However, there can be very defined muscular imbalances that are produced due to poor coordination of movement and timing resulting from environment, habit, motor control, poor proprioceptive awareness etc… that can carry over to the walking/running gait. These muscular imbalances can create dominances in certain muscles leading to a crossover gait for example. In a crossover gait the hip adducts during swing phase which can facilitate the hip flexors that internally rotate the femur (TFL) leading to excess hip adduction and internal rotation during stance. Now, as a result of this hip adduction and internal rotation dominance the psoas muscle, which is a hip flexor and external rotator, is going to have a less than optimal mechanical advantage at this point to help coordinate triple flexion.
2. I wish that we would stop getting hung up on these antiquated views of Kendall and Sahrmann “faulty” posture. Static posture has a poor link to dynamic function and is certainly not related to pain.
Static posture alone will tell you nothing. But static and dynamic posture, along with a detailed assessment gives the clinician a window into how the athlete’s brain represents movement and their ability to control and overcome gravity. You as a clinician know that we are always looking for patterns, whether optimal/suboptimal, that contribute to muscular imbalances. If someone is standing with a posterior COM, knees hyper-extended, hypertonicity in the quads, femoral medial rotation, with tibial lateral rotation, and has poorly defined gluts (“flat butt syndrome/gluteal amnesia”), I am going to start developing clinical hypotheses that I need to rule in/out during my assessment. Do I stop there and start treating, absolutely not, but it is a part of my clinical reasoning process. I think you would agree that the neuromuscular system wants to produce movement in the most efficient way possible. With that said, that does not always mean that it is biomechanically efficient. The human body will compromise quality of movement in order to conserve energy. This can be a big problem for an athlete if not addressed.
Now back to our assessment, once this same athlete starts to walk they begin to express that same quad dominant pattern with excess femoral medial rotation and poor loading response knee flexion with a limited ankle rocker. They single leg squat, hop, and jump with this same pattern. Why would their brain want to express any other pattern in an activity that is 2.5 to 2.8x body wt on one leg (running)? You have seen this same athlete running with excess hip adduction uncompensated pelvic drop, femoral medial rotation, and tibial lateral rotation (sign of the toes). This runner is extremely compliant to gravity and demonstrates poor muscular stiffness globally. Does giving this runner glut and core exercises alone change their muscular imbalances, absolutely not? I want this athlete just to start controlling gravity in all areas of life, let alone running. I want this athlete to understand what it is like to walk correctly and control and overcome gravity at 1.5x body weight. I want this athlete to be able to coordinate basic fundamental patterns of movement easily and then transfer that understanding to their running gait. This is the art/science of the clinician. Do we need to improve on our understanding of all aspects of human movement, absolutely! People like yourself, Tim Dorn, and countless other researchers, clinicians, and coaches need to keep up this discussion to further our understanding of the running athlete.
Thank you for your great work!!
Jeff Moreno
Thanks Jeff,
I think these discussions are important and interesting. I hope you don’t find it too Monday morning quarterbacking. I know no better way than to learn something than to discuss and question our own biases. Many call this Grad school.
While I like to get into the details academically I take the approach that the body is so incredibly complex that WE actually need to be much simpler in our interventions. Your posture response showed that. You don’t rely on the posture you probably place greater value in how they move. I’ve just taken this a little further in that I put very little value in the static assessment and mostly look at their running. I’m not even sure any simplistic tests of function (single leg squat – although I do it) really correlate with the kinematics that occur during running.
Your other two examples (limited ankle DF = limited hip extension) and the Jeptoo Valgus gait possibly causing a weakened Psoas because the psoas must shorten due to hip internal rotation) are interesting. You use observed kinematics to visualize where the psoas might be on its length tension relationship and then extrapolate how its force production might decrease.
So with those two examples its the “altered” positioning of the thigh during stance that lead to a conclusion of changes in active/passive hip torque.
Do you have any other kinematic flaws during running that you look for that might compromise psoas function?
Email if easier. Would love to continue the conversation. (I’m serious about testing it if you like: greglehmanphysio@gmail.com)
Quick follow up:
You wrote that the psoas is a flexor and EXTERNAL rotator of the hip – I misread that. Two points then:
1. If the hip internally rotates with the cross over gait than this would put the psoas under tension. This would then allow it to produce more force. Much like hip extension allows it to stretch and then release its energy.
2. I thought the psoas was a hip INTERNAL rotator. This is from Neuman’s article in 2010 on the Kinesiology of the hip muscles. Its moment arm is quite small (thats why i think it is pretty debatable). Not sure if you think this influences your theory or not. In some ways it might actually help it (via the length tension route) but it would lessen or insight into viewing hip internal rotation as an indicator of less psoas contribution to hip flexion.
Fun stuff!
Greg
Nice piece Jeff. Good to read someone who is stepping up and presenting something more they believe in, instead of just “Monday morning quarterbacking”/criticizing other ideas. It’s much easier to tell people what they’re doing wrong instead of putting out better ideas. Kudos to you.
I read Bosch and Klomp’s book back in the day. Wayyyyy back in 2005 ;-) I agree that the footstrike is set up by the motion of the preceeding swing phase. In addition, they say in their book that the strength of the swing assists the extension in the contralateral limb, “This scissor movement is nothing more than a combination of the stumble and inverse-extension reflexes. In other words, the bending of the hip and knee of one leg strengthens the extension in the other hip and knee and vice versa…the movement of the trailing swing leg ‘chases’ that of the leading leg involuntarily.” I wrote a bit about that last year on my blog.
Anyway, I enjoyed your piece and also enjoyed the DNS reference in the comments with the “punctum fixum.”
Good stuff!
Kevin- Thank you for your kind words. I think highly of you and your blog, and respect the quality of information that you post. I would love to post more often, but my busy schedule has limited me from doing so. How do you find the time?
We need more people like yourself posting on what is being done/seen in the clinic. We need those in the lab, those in the clinic, and those on the track/road doing amazing work talking too each other more often. Need to get people to understand normal movement!
“Normal Movement Produces Normal Healing”- Dan Pfaff
Would love to talk sometime about how you assess your running athletes.
Thanks Jeff. Email me anytime, love to talk about it.
Tim Dorn is doing some great research right now in gait. Take a look at his website some the great research articles that he has published.
I happen to disagree with some of his comments and would be interested in what others treating runners think. However, if you are a running geek like myself he has a great website. Check it out!
Hi Jeff,
Nice to meet you! I read your article with interest. In general, I believe that the (much) older research does not provide a clear assessment of the underlying mechanisms of running, primarily for two reasons:
1) You cannot make a running injury or strategy assessment from kinematics alone. There are many possible muscle recruitment strategies that can make up a given running motion because the human musculoskeletal system is overactuated (i.e. many more muscles than joints). We really need more work to determine what the real objectives of human running are. In other words, what are the low level criteria that we seek to achieve that makes us run the way we run. You may be interested in some recent work I presented this year on this topic: link to timzone.net and the accompanying video link to timzone.net
2) You cannot probe the kinetics of the musculoskeletal system. Given that it is not possible to non-invasively measure internal muscle or joint forces in the body during a dynamic activity, we must rely on computer models and simulations to generate predictions. Although our models aren’t perfect (and in general, not patient specific), we can still nevertheless probe internal metrics that can give us much more insight to how muscle groups synergize to coordinate movement. In a study last year (link to timzone.net), we found that the coordination strategies of running appear to be more complex than the eye suggests. Specifically, not only are the stance and swing phases of a leg highly correlated, but the forces in the ipsilateral leg significantly and simultaneously affect the dynamics of the contralateral leg (via the dynamic coupling effect). Although it may appear counter-intuitive at first glance, it actually makes a lot of sense because forces from a single muscle are transmitted through the joints along the entire body, and preparing one leg for some given part of the stride may require the other leg to be in a specific pose — thus requiring action to be taken by the contrilateral leg for the ipsilateral leg to function properly. I agree with your suggestion to “look globally” because everything is related to everything else and forces in the muscles must be generated at the precise times — this is why it’s so difficult to create walking robots — walking and running is more complicated than we think!
Of course, you are welcome to browse through all the articles on my website, http://www.timzone.net, including some hamstring injury papers during the late swing phase of sprint running, which you may find interesting. They all use musculoskeletal modeling and simulation to answer questions that cannot be answered from kinematic analysis alone. Feel free to post these comments on a blog if you so desire.
Cheers,
Tim
In a perfect world we would know all of the forces involved and the muscle activation patterns of each runner that we treat. Maybe that will happen someday, but not possible now, and the tech needed to be able to model forces internally is prohibitively expensive for most small clinics (and probably a lot of larger ones). I think we can infer some information about forces by looking at kinematics based on the lit available, and I certainly think there is value in a kinematic assessment in a clinical setting.
Another great post. This is exactly what I teach most of the injured runners I see for all sorts of reasons. The crossed extensor reflex is the basic movement pattern that we are trying to enhance. I find many ‘running schools’ are teaching people to be inactive at the hips. Unfortunately this is great for my business as reducing load at the hips causes an increased load in the lower leg often resulting in overload syndromes and injury. Some of the most common running cues I use to achieve what Jeff is talking about-greater hip flexor/extensor activation and antigravity movement can be found on the links below.
link to informrunning.com
link to informrunning.com
Glad to read of a similar approach
John Foster
John-I look forward to reading your blog. Sounds like you are doing some great work, look forward to learning from you!
Jeff Moreno
Brilliant and well written. I have worked as an ATC and currently as an MD. I do have some exposure to runners but more from an imaging perspective as an athlete. I have however encountered a significant number of patients who approach me for medical advice due to my hobby as a runner. I have always appreciated the whole body approach to problem solving and understanding the entire kinetic chain, literally from head to toe as opposed to focusing on foot strike alone or hip extension alone, etc…Thank you for the time in putting this together.
Glad you liked it! Any questions don’t hesitate to ask!
Glad you liked it. Any questions don’t hesitate to asked!
James- Thank you for the reference!